Introduction
The tool is based on the 'A guideline to assist healthcare professionals in the assessment of children and young people who may have an abdominal tumour'. The guideline has been developed following careful consideration of the available evidence through a systematic review and has incorporated professional expertise via a Delphi consensus process. You can also access the full guideline, and a summary version will be produced shortly.
Click on the symptoms below to navigate individual sections of the guideline and our recommendation to either Refer/Review/Reassure.
Key symptoms
Abdominal tumours encompass a large number of different tumours, namely Wilms’ tumour, neuroblastoma, hepatoblastoma, abdominal lymphomas, soft tissue sarcomas and germ cell tumours.
The following symptoms and signs are all associated with childhood abdominal tumours. Their presence should alert the clinician to this possibility.
Core symptoms
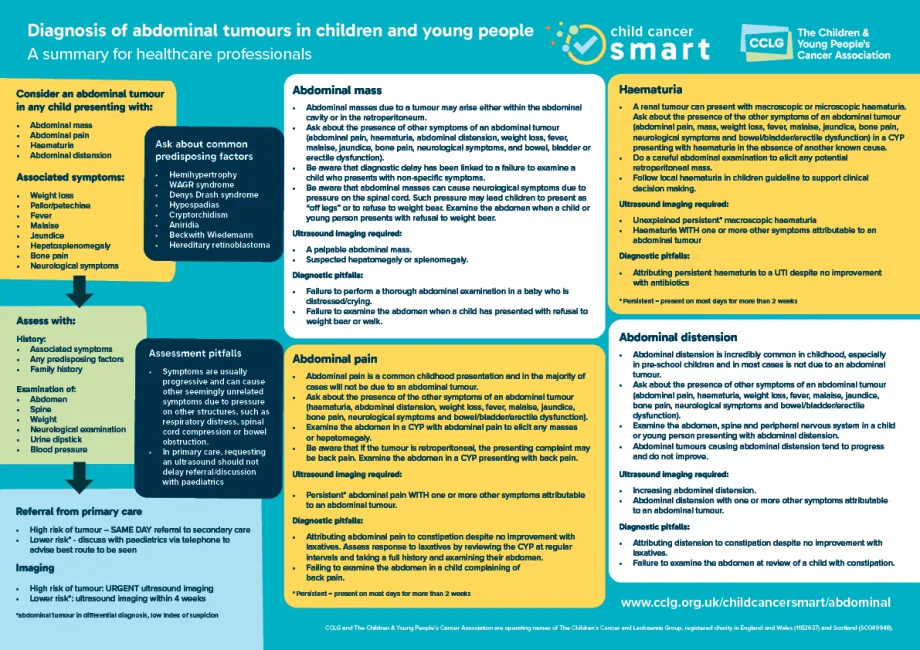
- Abdominal mass
- Abdominal pain
- Haematuria
- Abdominal distension
Associated symptoms
- Weight loss
- Pallor/ petechiae
- Fever
- Malaise
- Jaundice
- Hepatosplenomegaly
- Bone pain
- Neurological symptoms from spinal cord compression
- Bladder/bowel/erectile dysfunction due to spinal cord compression
- Urinary retention
Associated symptoms are dependent on the type of tumour and it is important to ask for the presence or absence of the associated symptoms.
Predisposing factors
Ask about common predisposing factors associated with an increased risk of childhood abdominal tumours:
- Hemihypertrophy
- WAGR (Wilm's tumor, aniridia, genito-urinary abnormalities, and mental retardation) syndrome
- Denys Drash syndrome
- Hypospadias
- Cryptorchidism
- Aniridia
- Beckwith Wiedemann
- Hereditary retinoblastoma
Verify the presence of predisposing factors with parents/patients as they may lower the threshold for referral and investigation.
1. Abdominal mass
- Ask about the presence of the other symptoms of an abdominal tumour (abdominal pain, haematuria, abdominal distension, weight loss, fever, malaise, jaundice, bone pain, neurological symptoms and bowel/bladder/erectile dysfunction).
- Be aware that abdominal masses can cause neurological symptoms due to pressure on the spinal cord. The pressure can cause children to present as “off legs” or refusal to weight bear. Examine the abdomen when a CYP presents with refusal to weight bear.
This tool works best on desktop, or by rotating your phone to horizontal
| Symptoms | Actions | |
| Reassure |
|
|
| Review |
|
|
Refer
|
|
|
- Failure to perform a thorough abdominal examination in a baby or toddler who is distressed/crying
- Failure to examine the abdomen when a child has presented with refusal to weight bear or walk.
- Failure to reassess the abdomen after treating for constipation
History
Take a detailed history, including the presence or absence of the other symptoms on the list above, history of injury, predisposing factors and a family history for CYP presenting with symptoms suggestive of an abdominal tumour.
Assessment
- Abdominal examination
- Spinal examination
- Weight
- Neurological examination
- Urine dipstick
- Blood pressure
Assessment pitfalls
Symptoms are usually progressive and can cause other seemingly unrelated symptoms due to pressure on other structures, such as respiratory distress, spinal cord compression or bowel obstruction.
- Respiratory distress
- Symptoms/sign of spinal cord compression
2. Abdominal Pain
- Abdominal pain is a common childhood presentation and in the majority of cases will not be due to an abdominal tumour
- Abdominal pain without any other symptoms is very unlikely to be due to cancer.
- Ask about the presence of the other symptoms of an abdominal tumour (haematuria, abdominal distension, weight loss, fever, malaise, jaundice, bone pain, neurological symptoms and bowel/bladder/erectile dysfunction).
- Be aware that if the tumour is retroperitoneal, the presenting complaint may be back pain. Examine the abdomen in a CYP presenting with back pain.
This tool works best on desktop, or by rotating your phone to horizontal
| Reassure |
|
|
| Review |
|
|
| Refer |
|
|
- Attributing abdominal pain to constipation despite no improvement with laxatives. Assess response to laxatives by reviewing the CYP at regular intervals and taking a full history and examining their abdomen.
- Failure to examine the abdomen in a child complaining of back pain
*Persistent = present on most days for more than 2 weeks
History
Take a detailed history, including the presence or absence of the other symptoms on the list above, history of injury, predisposing factors and a family history for CYP presenting with symptoms suggestive of an abdominal tumour.
Assessment
- Abdominal examination
- Spinal examination
- Weight
- Neurological examination
- Urine dipstick
- Blood pressure
Assessment pitfalls
Symptoms are usually progressive and can cause other seemingly unrelated symptoms due to pressure on other structures, such as spinal cord compression or bowel obstruction.
- Abdominal pain waking them at night
- Associated back pain
3. Haematuria
- A renal tumour can present with macroscopic or microscopic haematuria
- Ask about the presence of the other symptoms of an abdominal tumour (abdominal pain, mass, weight loss, fever, malaise, jaundice, bone pain, neurological symptoms and bowel/bladder/erectile dysfunction) in a CYP presenting with haematuria in the absence of another known cause.
- Do a careful abdominal examination to elicit any potential retroperitoneal mass.
- This decision support tool should be used in conjunction with your local haematuria in children guideline.
This tool works best on desktop, or by rotating your phone to horizontal
| Symptoms | Actions | |
| Reassure |
|
|
| Review |
|
|
Refer
|
|
|
Attributing a persistent* haematuria to a UTI despite no improvement with antibiotics
*Persistent = present on most days for more than 2 weeks
History
Take a detailed history, including the presence or absence of the other symptoms on the list above, history of injury, predisposing factors and a family history for CYP presenting with symptoms suggestive of an abdominal tumour.
Assessment
- Abdominal examination
- Spinal examination
- Weight
- Neurological examination
- Urine dipstick
- Blood pressure
Assessment pitfalls
Symptoms are usually progressive and can cause other seemingly unrelated symptoms due to pressure on other structures, such as spinal cord compression or bowel obstruction.
- Hypertension
4. Abdominal distension
- Abdominal distension is incredibly common in childhood, especially in pre-school children.
- In most cases abdominal distension is not due to an abdominal tumour.
- Abdominal tumours causing abdominal distension tend to progress and does not improve.
- Ask about the presence of the other symptoms of an abdominal tumour (abdominal pain, haematuria, weight loss, fever, malaise, jaundice, bone pain, neurological symptoms and bowel/bladder/erectile dysfunction).
This tool works best on desktop, or by rotating your phone to horizontal
| Symptoms | Actions | |
| Reassure |
|
|
| Review |
|
|
Refer
|
|
|
- Attributing distension to constipation despite no improvement with laxatives
- Failure to examine the abdomen at review of a child with constipation
History
Take a detailed history, including the presence or absence of the other symptoms on the list above, history of injury, predisposing factors and a family history for CYP presenting with symptoms suggestive of an abdominal tumour.
Assessment
- Abdominal examination
- Spinal examination
- Weight
- Neurological examination
- Urine dipstick
- Blood pressure
Assessment pitfalls
Symptoms are usually progressive and can cause other seemingly unrelated symptoms due to pressure on other structures, such as spinal cord compression or bowel obstruction.
- Hard distended abdomen with or without distended veins
- Progressively increasing distension
- Associated vomiting and/or constipation
- Not resolving with laxative therapy
Summary poster